Using Community-Centered Root Cause Analysis to Reach the Last Mile in NTD Elimination
By Dany Chhan, WI-HER Senior Associate

A health worker in Uganda offered Julius Otim* medicine that prevents and treats trachoma infection, but he refused to take it.
Trachoma is an eye disease that causes blindness or visual impairment around the world, including among people in Julius’ town of Moroto, Uganda. It is transmitted by flies and infected surfaces like hands and clothes that have been in contact with the bacterium Chlamydia trachomatis. Trachoma can be prevented by taking antibiotics, which are often distributed by health workers to entire at-risk communities at the same time via mass drug administration (MDA). Maintaining facial cleanliness, as well as good hygiene and sanitation, are also vital to prevent the spread of the disease.
“In my family,” Julius said, “there was a belief that our relatives got blind because of a curse caused by one of the cows used to marry my great-grandmother. This cow is said to have been blind.” Because he did not understand how trachoma spreads or how to prevent it, Julius refused to take the preventive medicine when the health worker offered it to him.
Misconceptions like those in Julius’ family are common in communities that face the devastating effects of neglected tropical diseases (NTDs). People’s misconceptions, information gaps, and fears about NTD causes and prevention techniques contribute to continued NTD transmission in some communities. Other factors, such as systematic challenges in access to health care and lack of community acceptance of MDA, also contribute to the continued prevalence of trachoma in Uganda.
Root cause analysis (RCA) is a process for assisting programs in rapidly identifying populations that are being missed with interventions and barriers they are experiencing. Through community RCA, programs learn why these populations are not participating in order to facilitate targeted, localized action.
A root cause analysis (RCA) helps identify gaps in the health system and considerations around gender, socioeconomic status, livelihood, ethnicity, religion, and disability that serve as barriers to communities accessing and accepting NTD services. These barriers are common among the most marginalized populations and communities, as they experience overlapping and diverse forms of vulnerability and identity, such as conflict-affected populations, Indigenous and migrant communities, cross-border groups, youth, women, and ethnic minorities. Many of these populations inhabit a country’s proverbial “last mile” of NTD elimination. Only by understanding and addressing the reasons why individuals and communities miss or choose not to take NTD preventive medicine can governments strive to achieve the WHO’s target to prevent, control, and eliminate NTDs by 2030.
What a Root Cause Analysis Tool is & Its Role in Behavior Change Activities to Reach the Last Mile
Recognizing that rapid assessment and localized action is increasingly needed in NTD elimination, USAID’s Act to End Neglected Tropical Diseases | East (Act | East) program worked with governments to conduct assessments to better understand the constraints and opportunities to improve MDA coverage in five countries, Ethiopia, Haiti, Nepal, Tanzania, and Uganda. To operationalize the assessment recommendations, Act | East works with local stakeholders to apply an RCA tool as part of WI-HER’s iDARE™ methodology to ultimately co-design and expand local solutions with the groups most often missed or excluded by NTD services.
The Root Cause Analysis tool and overarching implementation process serve as a bridge between larger-scale assessment and targeted programmatic action (Figure 1).
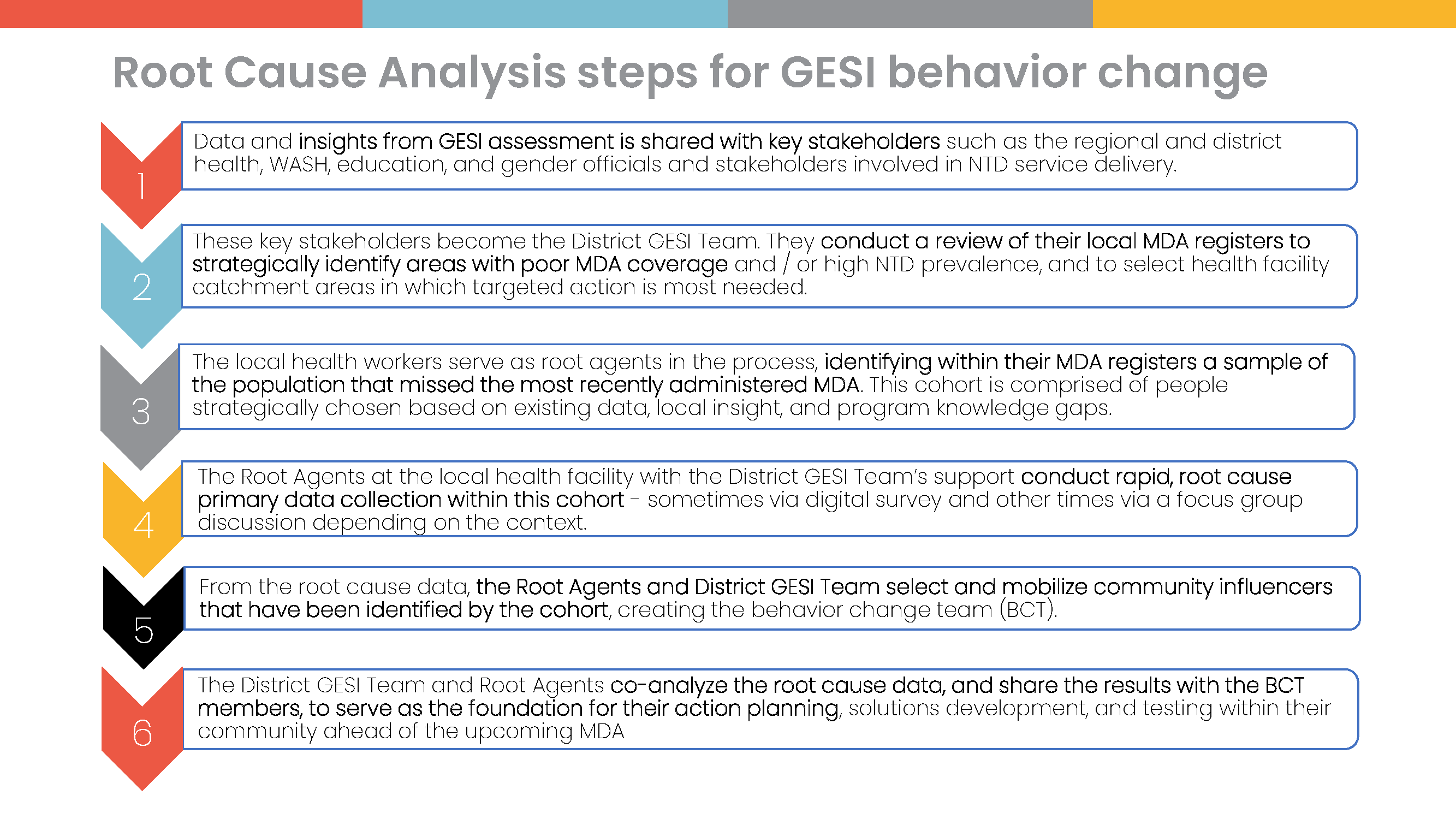
The RCA tool includes questions on perceived norms, attitudes, beliefs, and influencing factors that shape the respondent’s decision to participate in MDA. Local health officials typically deploy the tool among a sample of the local population who missed taking the medicine in the previous MDA. The results give local officials insight into who precisely missed the previous MDA and why.

In response, influential stakeholders, such as religious leaders, local political and cultural leaders, male and female elders, teachers, business persons, and local health workers, can design and implement action plans to address the reasons for low MDA uptake identified through RCA. Using these data and action plans, district health officials engage in strategic planning for regional and district-wide MDA and microplanning at the sub-district level. As a whole, this rapid assessment results in an enhanced understanding of context and location-specific coverage issues that foster locally owned and implemented solutions.
In Moroto, Uganda, root agents used the RCA tool to ask community respondents who contributed to their health decision-making, and many respondents named Julius Otim as an influencer. The Moroto district health office then equipped Julius and other community-endorsed influencers to address the RCA findings ahead of the next trachoma MDA.
Julius shared, “Following my selection as an influencer and the trachoma training I received, I was able to understand all the signs and symptoms of trachoma, and these are the same I saw with our relatives who became blind. With this information, I was able to mobilize my relatives for MDA, telling them blindness in our family was not caused by a curse but untreated trachoma.”
Julius worked within his family and larger community to share accurate information about trachoma and its prevention ahead of the next medicine distribution. Addressing the specific misconceptions that the RCA identified as prevalent in that area, Julius, for example, counseled charcoal burners and mobile workers, who the RCA identified as more likely to be missed by MDA. Interactions like these highlight the power and necessity of identifying the root causes of NTD program challenges and crafting solutions grounded in this community context.
3 Country Examples: How RCA was Used to Strengthen MDA Planning and Implementation
Ethiopia
In 2022, Act | East partnered with woreda health officials to implement a Root Cause Analysis in Adaba woreda in Ethiopia’s Oromia region due to challenges with MDA coverage. The RCA data identified several reasons, commonly expressed by the respondents, why the woreda was not reaching the minimal MDA coverage of 80%:
- general low awareness levels of MDA hindered acceptance,
- a lack of door-to-door services to reach remote communities resulted in missing key groups, and
- seasonal activities prevented community members from being available in the district during MDA.
The RCA data also identified other key reasons why local community members missed or did not participate in MDA, including a fear of side effects and misinformation about the medicine.
Equipped with this deeper understanding, capacitated community influencers developed solutions focused on awareness raising, such as updating pre-MDA messaging and sources (i.e., town criers, outreach to schools) and tailoring messages to youth via social media. The woreda health officials shared the additional findings regarding MDA timing and distribution method at the region’s MDA planning meetings to shape the overall strategy of MDA. As the woredas scaled up these solutions, Adaba experienced marked improvements in MDA coverage. For example, the MDA coverage increased from 75% in 2021 before the activity began to 92% coverage in 2023, propelling the woreda to achieve the MDA coverage requirements.
Nepal
In Banke’s Ward 3, the ward health officials conducted RCA in 2022 with a sample of the population who did not take the previous MDA and had been identified through reviewing MDA registers. In total, 32.2% of this cohort stated that they did not take the last MDA because they did not have health problems associated with lymphatic filariasis (LF) and, therefore, they thought they did not need to take the drug. Additionally, 34.3% named fear of the medicine’s side effects as the main reason they did not participate in the previous MDA. Further analysis showed that over 50% of the female cohort members credited mobility restriction and 43% lack of decision-making power, respectively, as the reasons why they missed MDA. To address these barriers, influencers in the community focused their efforts on building relationships and trust with cohort members, especially those with restricted movement outside the home, via repeated house visits to dispel myths and raise awareness about MDA and LF. Such solutions to local barriers identified in the RCA led to the development of a Nepal Social Mobilization Guide, which will be used as a resource in future MDA planning.

Uganda
Recommendations and insights from RCA strengthen MDA planning and implementation, ultimately reaching more people with MDA services. For example, during implementation in Nabilatuk District in 2022, the RCA revealed that a high number of migrant farmers missed the previous MDA due to their migration to a neighboring district, Napak. The District GESI team shared this information during an MDA microplanning meeting to emphasize that coordination between Nabilatuk and Napak was needed to address this challenge. District officials in Nabilatuk then liaised with Napak District to train and supervise community medicine distributors to provide medication to migrant farmers. As a result, the program reached 9,672 people in Nabwal Sub-County in Napak, covering 87% of the sub-county’s population targeted for treatment.
Through these examples, it is clear that RCA is a valuable and necessary tool to understand barriers to access and acceptance of MDA, especially when those barriers are related to gender and social exclusion factors. Achieving overall health equity and eliminating NTDs by 2030 depends on delivering services and reaching the ‘last mile.’ Root cause analysis is an essential tool in these efforts.
* Names have been changed throughout to protect the privacy of the individuals.