Working Together: A Regional Approach to Improving Skin-to-Skin Contact and Well-baby Care in the Eastern and Southern Caribbean
By Morgan Mickle, Gender Specialist, WI-HER, LLC
“A third of low birth weight babies die within the first twelve hours after delivery, largely because they get cold very quickly, causing them to stop feeding and leaving them more susceptible to infection.” – Maternal and Child Survival Program 1
Skin-to-skin contact immediately after birth between baby and family members, particularly mothers, can lead to improved health outcomes for both child and mother, yet the practice is underutilized in many countries. Skin-to-skin contact refers to placing a newborn baby naked (and not wrapped in a blanket) on the mother’s (or substitute person’s) chest or abdomen immediately after birth (and continued periodically). Studies have shown that skin-to-skin contact helps regulate the baby’s temperature (preventing the risk of hypothermia) and heart and breathing rates, making them more stable and exhibiting vital signs at healthy neonate levels23. It also helps elevate the baby’s blood sugar and helps build its immune system by exposing the baby to the same bacteria as the mothers’. Beyond these early health accomplishments, babies who receive skin-to-skin contact could be happier as bodily contact helps reduce pain and stress levels, and also leads them to cry less4.
Holding babies skin-to-skin also supports a baby’s brain development and helps facilitate early breastfeeding. Babies who are kept skin-to-skin with the mother immediately after birth for at least one hour are more likely to latch on (and well) to the nipple for breastfeeding without any assistance, allowing the baby to get milk more easily. One study showed that when a newborn is placed skin-to-skin with its mother, the newborn is more likely to exhibit specific behaviors that lead to first breastfeeding, often within the first hour after birth5.
Mothers benefit from skin-to-skin contact with their babies after birth too. Research has demonstrated that mothers who hold their newborns skin-to-skin have increased maternal behaviors, such as kissing their infant more and looking into their infant’s faces, show more confidence in caring for their baby, and breastfeed for longer periods of time. Mothers who hold their babies skin-to-skin also help reduce the negative effects of separation from mothers that babies may experience. Additionally, fathers also benefit from skin-to-skin contact. Studies have shown that fathers who practice skin-to-skin contact with their newborns demonstrate increased exploring, talking, touching, and caring behaviors with the child. The experience enhances father-neonate attachment and promotes parental confidence6.
In the context of Zika response programming, skin-to-skin promotion at the facility level not only helps boost the health status of all newborns, but also can facilitate bonding early on between parents and children.
If the practice of skin-to-skin contact provides such important health benefits for both mom and baby, why are initiation rates so low?
From March 25-27, 2019 the USAID ASSIST Project, with support from its partners WI-HER and the American Academy of Pediatrics, led a Regional Meeting among health practitioners and managers from 4 countries across the Eastern and Southern Caribbean. The purpose of the meeting was to provide a platform for further training, knowledge exchange, and strengthening the collaboration among health leadership across the region. Hosted in St. Kitts and Nevis, and attended by a USAID representative from the Eastern and Southern Caribbean Regional field office, the platform brought together over 50 representatives from the host nation, Antigua and Barbuda, Dominica, and St. Vincent and the Grenadines. Country teams comprised of top-performing health centers and hospitals, quality improvement coaches, and Ministry of Health champions and focal persons.
Over the course of the three-day meeting, participants identified low rates of skin-to-skin contact as one of the main challenges they face. Under the ASSIST project, hospital facilities monitor and document any occurrence of hypothermia in newborns. As part of their quality improvement practices, hospitals seek to reduce rates of hypothermia through promotion of skin-to-skin contact.
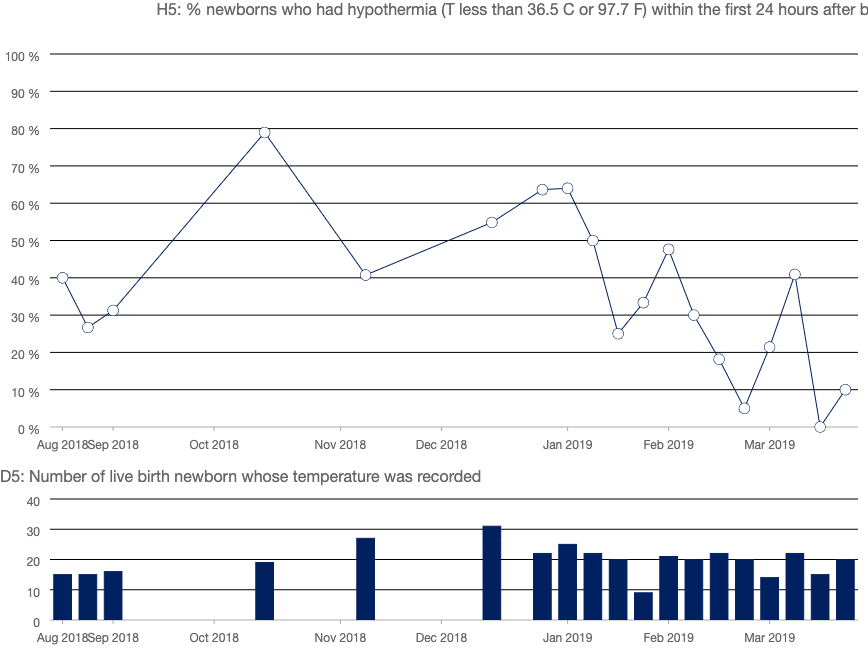
Source: USAID ASSIST Project indicator database (IID)
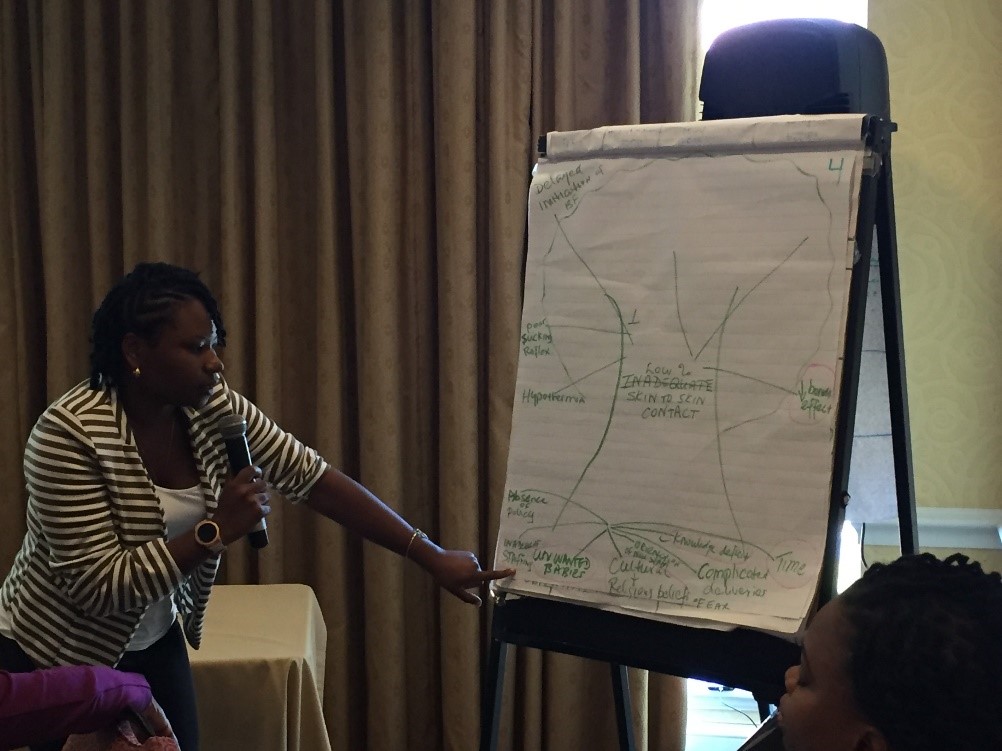
Representatives from WI-HER led gender sensitization training and facilitated the exchange of information around best practices to improve skin-to-skin contact. Through team activities aimed at exploring obstacles to best practices, participants identified knowledge deficit as a root cause of low skin-to-skin contact at birth.
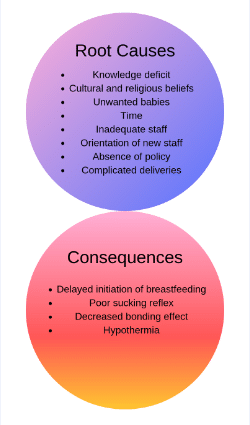 Participants noted that both providers and beneficiaries (mothers, family members, caregivers) need exposure to information and/or training on the benefits of skin-to-skin contact and the risks of hypothermia. In addition, the health teams identified resistance to change among providers, inadequate or new health staff, lack of policies, and non-user-friendly manuals and guides as potential obstacles to successfully implementing solutions.
Participants noted that both providers and beneficiaries (mothers, family members, caregivers) need exposure to information and/or training on the benefits of skin-to-skin contact and the risks of hypothermia. In addition, the health teams identified resistance to change among providers, inadequate or new health staff, lack of policies, and non-user-friendly manuals and guides as potential obstacles to successfully implementing solutions.
To overcome these challenges, the multi-country teams advocated for education, the development and implementation of facility policies requiring skin-to-skin contact at birth, and the orientation and reorientation of health staff. Tracking improvements in the quality of services will help to reinforce new practices and boost staff morale in their commitment to sustain the improvements.
Though solutions will need to fit each local context, the sharing of knowledge through regional meetings like this promote awareness and stimulate change. It is hoped that collaborative problem-solving will lead to sustainable improvements that will increase skin-to-skin contact at birth and improve the health of newborns and families.
From 2012-2017, the USAID ASSIST (Applying Science to Strengthen and Improve Systems) Project fostered improvements in 38 countries in a range of health care processes through the application of modern improvement methods by host-country providers and managers and build the capacity of host-country systems to improve effectiveness, efficiency, client-centeredness, safety, accessibility, and equity of the health services they provide. In a two-year extension from 2017-2019, ASSIST applies quality improvement methods to health systems strengthening efforts in Zika-affected countries, including Antigua and Barbuda, Dominica, Dominican Republic, Ecuador, El Salvador, Guatemala, Honduras, Jamaica, Nicaragua, Paraguay, Peru, St. Kitts and Nevis, and St. Vincent and the Grenadines.
WI-HER, LLC (Women Influencing Health, Education and Rule of Law) is a woman-owned small business that partners with international donors, national governments, non-governmental organizations and others to identify and implement creative solutions to complex development challenges to achieve better, healthier lives for women, men, girls, and boys. Founded by Dr. Taroub Harb Faramand in 2011, WI-HER, LLC works to integrate gender through contextualized, adaptable, and systems strengthening methods that can be seamlessly integrated into ongoing and new programs. WI-HER is committed to ensuring equal opportunities for women, men, girls, and boys, as well as all other vulnerable groups, including LGBTQI+ people.
- Maternal and Child Survival Program. Kangaroo Mother Care. https://www.mcsprogram.org/our-work/newborn-health/kangaroo-mother-care/
- Phillips, Raylene. Uninterrupted Skin-to-Skin Contact Immediately After Birth. NAINR. 2013. https://www.researchgate.net/publication/257612445_The_Sacred_Hour_Uninterrupted_Skin-to-Skin_Contact_Immediately_After_Birth.
- Newman, Jack. The Canadian Breastfeeding Foundation. The Importance of Skin to Skin Contact. 2009. https://www.canadianbreastfeedingfoundation.org/basics/skin_to_skinb.shtml
- Gray, Larry et. al. Skin-to-Skin Contact Is Analgesic in Healthy Newborns. Pediatrics. 2000. https://pediatrics.aappublications.org/content/pediatrics/105/1/e14.full.pdf?ck=nck
- According to Dr. Widstrom and the video Skin to Skin in the First Hour After Birth: Practical Advice for Staff after Vaginal and Cesarean Birth by the Healthy Children Project, the nine instinctive stages include 1) the birth cry, 2) relaxation, 3) awakening, 4) activity, 5) resting, 6) crawling, 7) familiarization, 8) suckling, and 9) sleeping.
- Chen, Er-Mei, et. al. Effects of Father-Neonate Skin-to-Skin Contact on Attachment: A Randomized Controlled Trial. Nursing Research and Practice. 2017. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5282438/