Children with Congenital Syndrome associated with Zika and the importance of addressing gender factors that limit their adherence to their therapeutic plan: The case of Paraguay
By Marlene Espinola y Andrea Ruffinelli, Technical Facilitators for ASSIST Paraguay, Elga Salvador, Senior Gender Advisor, WI-HER, LLC
In response to the Zika epidemic, the USAID Applying Science to Strengthen and Improve Health Systems (ASSIST) Project in Paraguay has been collaborating with the Ministry of Public Health and Social Welfare (MSPyBS) to improve the capacity of health services to prevent Zika during pregnancy, screen cases of Zika infection among women of reproductive age and screen microcephaly and other symptoms of Congenital Syndrome associated to Zika (CSaZ) in newborn children. Additionally, ASSIST aims to strengthen the provision of high-quality psycho-emotional support services for women and families affected by Zika and increase the number and proportion of affected infants receiving recommended care.
On February 12 and 13, 2019, the Paraguay USAID Project team and representatives of the MSPyBS participated in a training workshop on gender integration into Zika programs, with the facilitation of the WI-HER Senior Gender Advisor, Elga Salvador.
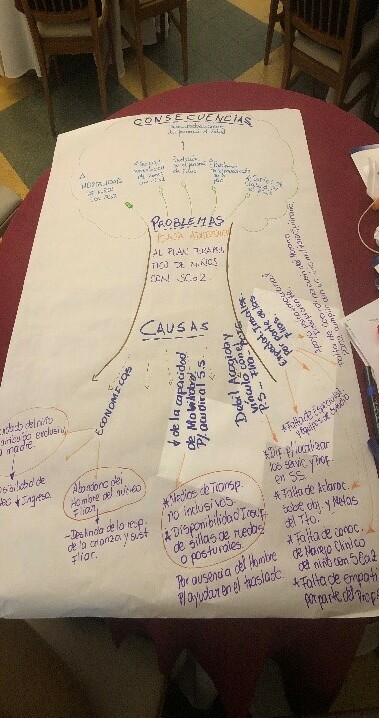
The training focused on sensitizing participants in gender themes and strengthening their capacity to identify and address gender factors in the Zika response that limit the results of the interventions in the health sector, both during antenatal care and postnatal care of children with CSaZ. The activity culminated with working groups that designed both new ideas for change aimed at addressing the identified gender gaps, and monitoring systems to analyze if and how improved health outcomes are achieved.One of the problems that the ASSIST technical assistants wanted to analyze in depth during this training was low adherence to comprehensive therapeutic treatment by children with CSaZ.Most of the children with CSaZ need to go to health centers periodically for diagnosis, analysis, specialized studies and visits, physical and occupational therapy, as well as early stimulation sessions. Non-adherence to a recommended therapeutic plan can have grievous consequences, such as: aggravating the symptoms of Zika and increasing the morbidity and mortality of infants with SCaZ; for family members, it can mean psycho-emotional disorders as well as increased out-of-pocket expenses; and for health professionals, this can lead to frustration. Therefore, it is crucial to have an in-depth understanding of gender-based factors that impede adherence to a child’s therapeutic plan and how to address them.According to the analysis conducted by one of the working groups during the February workshop, one of the main factors that limit adherence to the therapeutic plan of children with CSaZ is the family economic situation. Paying for medicines that are not covered by insurance, performing tests, conducting studies and specialized visits, periodically attending required follow-up visits, attending physical and occupational therapy, and traveling to health centers, …. all this incurs higher costs than the care of healthy children. In many cases, these expenses are associated with loss of financial income, because taking care of children with CsaZ requires much more time and attention, and mothers or other women in the family must leave income-generating jobs. All this would have a significant weight on family finances, but the situation is even more complicated when fathers of infants with CSaZ abandon the family. As often happens in Paraguay, the father may neglect to participate in the care of the child or to offer financial contributions to the family. This leaves the mother to assume both the role of caretaker and provider.
“[…] I could not go to the follow up visit because I did not have the money to pay for the bus transfer to the hospital […]” (Single mothers who have not gone to public hospitals in Alto Paraná, testimonies offered via telephone conversations).
The fact that childcare is attributed exclusively to mothers is also a factor that contributes to limited adherence of children with CSaZ to their therapeutic plans. The health personnel who care for children with CSaZ estimate that more than 90% of the care of their basic needs, which includes, hygiene, nutrition, medical consultations and early stimulation exercises, is assumed exclusively by mothers or other women of the family. This is related to cultural norms that consider caregiving roles as feminine and that it is “natural” for a woman to perform domestic roles. On the contrary, it is considered “normal” that men cannot assume these roles, because they must engage in paid work as providers. In patriarchal societies, such as in Paraguay, these gender stereotypes are strongly rooted; they continue to be socialized within families, including through the teachings of mothers and grandmothers, within schools and other areas of the society.
As one can hear every day in Paraguay, “Upeicha nte ara voi“, which translated from Guarani into English as ” That’s how things are.” In fact, to meet these expectations, most mothers of children with CSaZ end up dedicating themselves full-time to household chores and to the care of these children. On the other hand, it is not only men who do not involve themselves in care; but in many cases the same women think that their male partners cannot collaborate on these tasks. This is illustrated in a conversation between a health provider and a mother of a child with CSaZ who attends the high-risk clinic of the Regional Hospital of Ciudad del Este (HRCDE).
“[…] you come alone?” (Health provider).
“Yes. His father is working and does not take care of him, then … “(Mother of a child with CSaZ).
“But is it because he does not want to?” ((Health provider).
“No, it’s because he does not understand him. He does not know how to take care of him; we, women only understand our children […] “(Mother of a child with CSaZ).
In this same center, of the six children with CSaZ who regularly attend their consultations, only one is accompanied by the father. The others are accompanied by the mothers or other women of the family, such as grandmothers or aunts.
It is important to highlight that fulfilling traditionally assigned gender roles to attend to all household tasks and to take care of all family and children with special needs; mothers of children with CSaZ often experience situations of stress, frustration, anxiety, and sometimes they are unable to accompany their children to their appointments.
In addition to economic factors and deeply rooted gender norms in the local culture, participants in the workshop analyzed other factors internal to the health system that hinder the adherence of children with CSaZ to the comprehensive health plan and therapy. First, a series of logistical and structural factors were highlighted that undermine families’ expectations, affecting their motivation to go attend services. Some examples include limited number of specialists for child neurology and child phono-audiology, and that to receive their services or perform specialized tests it is necessary to go to hospitals equipped with appropriate personnel and equipment, which could involve traveling to other cities. Other factors include the lack of support and collaboration for the coordination of appointments at times that align with family needs; the lack of adequate psycho-emotional support counseling and services; and difficulty in locating services due to the lack of appropriate signs.
As in most of the countries in Latin America and the Caribbean region, the Paraguayan health system is focused primarily on women of reproductive age, pregnant women and children. In recent years there have been efforts to change and gradually incorporate men as primary recipients of health care; for example, with the recent creation of the Integral Health Program for Men and Women. Efforts are made also to promote male participation in the care for the health of their families. However, progress remains limited and both the portfolio of services and the health personnel continue to be oriented towards women and children. Since traditionally women, not men, attend health services both as clients and accompanying persons for children, both clients present in the waiting rooms and providers often have biased attitudes towards men who approach services, especially of sexual and reproductive health and pediatrics.
The attitudes of the health personnel, the unwelcoming environment and the lack of client-provider links, constitute other important factors that may dissuade adherence to care. Health personnel who do not have adequate sensitization and knowledge about Zika and gender, and lack specific training on the integral treatment of families of children with CSaZ, may have biased and discriminatory attitudes towards clients. Therefore, clients of the health services often report unwelcoming and unfriendly experiencing with health providers that affect a family’s motivation to regularly attend services and adhere to their infant’s therapeutic plan. Additionally, the lack of clear information about the therapy’s objectives, goals and benefits for child development also hinders adherence.
Based on this analysis and other considerations, the health personnel who participated in the training on gender integration of in the Zika context, reflected on how to address the factors mentioned above in order to promote greater adherence of children with CSaZ to their therapeutic plan. They proposed the following ideas for change:- Carry out sensitization activities for mothers, fathers and health personnel on the benefits of father participation in care on child development.- Through follow-up notebooks, send written invitations addressed to fathers of children with CSaZ to attend appointments.- During non-working hours, conduct information sessions aimed at fathers and men to increase their bond to their children and involve them in early stimulation activities.- Create of a network of support and communication between fathers of children with CSaZ.- Train health personnel on gender integration in family planning programs, prenatal care, postnatal care, pediatrics and health in general.- Strengthen the network of services and create a network of health providers that can guarantee access to established medical interventions.
Among these initiatives, male involvement in the consultations of children with CSaZ is fundamental for the optimization of treatment, the reduction of stress in the mother and the creation of closer family bonds. To achieve this, gender sensitization of health personnel and the production of gender-sensitive informative material and guidelines are key steps. These actions within the health sector can promote more gender equity in the services and, by promoting greater men’s participation, can increase adherence to treatment of children with CSaZ.
The promotion of male participation in these contexts is the responsibility of the health sector alone, rather it implies alliances with stakeholders outside of hospitals and a long-term intersectoral approach that transforms cultural paradigms about care within the families. With proper commitment and collaboration “Ko’a mba’e ikatu ñacambia”: things can change.